이달의 증례
| Application of retrograde pedal access, transcollateral and pedal-plantar loop approach in a young CLI patient with all BTK total occlusions. | |||
|---|---|---|---|
| 년도 | 2018년 6월 | ||
| 카테고리 | 이달의 중재술 | ||
| 저자 | Hee-jin Kwon / Jae-Hwan Lee | ||
| 소속 | Chungnam National University Hospital | ||
| 첨부파일 1 | 2.jpg | ||
- 관리자
- 등록일 : 2018.05.28
- Hit 1,837
A 34-year-old woman with a 1-pack year smoking history was referred to our hospital because of resting pain and gangrene at 2nd toe of her left foot (Fig. 1). The wound occurred a month ago and gradually worsened. She had no claudication. Femoral and popliteal pulse were palpable, but dorsalis and plantar pedal pulses were absent in her left foot. Ankle brachial indices were normal in both leg. Electrocardiogram (ECG) showed normal sinus rhythm and there was no specific finding in chest x-ray and laboratory test. Serologic markers of autoimmune disease yielded negative results. A computed tomographic angiogram revealed both BTK arterial occlusion. There were diffuse total occlusion of anterior tibial artery (ATA), peroneal artery (PA) and posterior tibial artery (PTA) on her left leg. No dorsalis landing zone was observed and the medial plantar artery was the only single landing zone in the foot.
{kind=link}
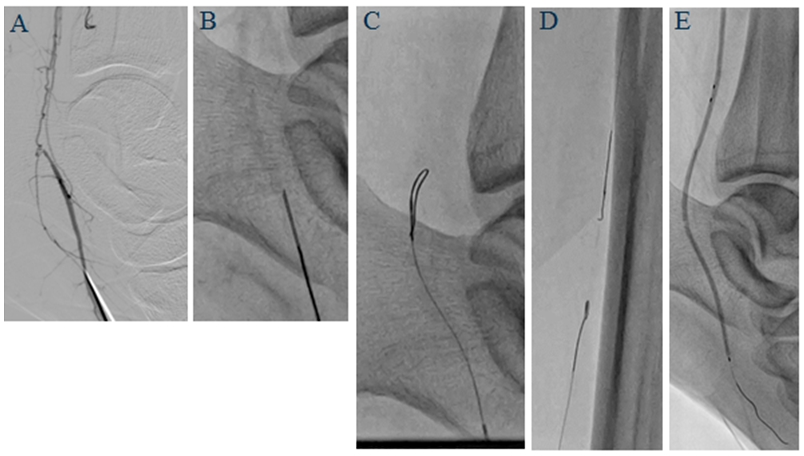
Since the antegrade approach of ATA CTO was failed at outside hospital (Fig. 2), we planned a retrograde approach for long PTA CTO lesion initially. The left common femoral artery (CFA) was punctured in antegrade direction and a 6Fr Ansel sheath was introduced to popliteal artery level (Cook company, US). An angiogram showed normal femoral and popliteal artery. But, whole BTK arteries were diffuse totally occluded. The ATA was diffusely occluded from the distal level without visible dorsalis artery. The PTA was also diffusely occluded from the proximal level to the common plantar artery. The medial plantar artery was the only landing pedal artery. And the PA showed totally occluded at the proximal level. There were plenty of corkscrew like collateral circulation noted. We tried to puncture the proximal medial plantar artery retrogradely with a 7cm, 21gauge needle (Fig.3-A,B). But, it was very difficult due to small artery size and deep location. On the first attempt, a command ES guidewire was advanced to vein. After a few tries, the artery was successfully punctured and sheathless approach was performed using a CXI and a command ES guidewire through subintimal space (Fig.3-C,D). Then based on retrograde guidewire, antegrade navigation of guidewire from proximal PTA was performed using an armada XT over-the wire (OTW) balloon and a Regalia guidewire, and successfully passed to medial plantar artery. Balloon angioplasty for left PTA was performed with a 2.5x80mm balloon catheter and 2.0/2.5x210mm tapered balloon catheter for whole PTA and medial plantar artery (Fig.3-E).
{kind=link}
{kind=link}
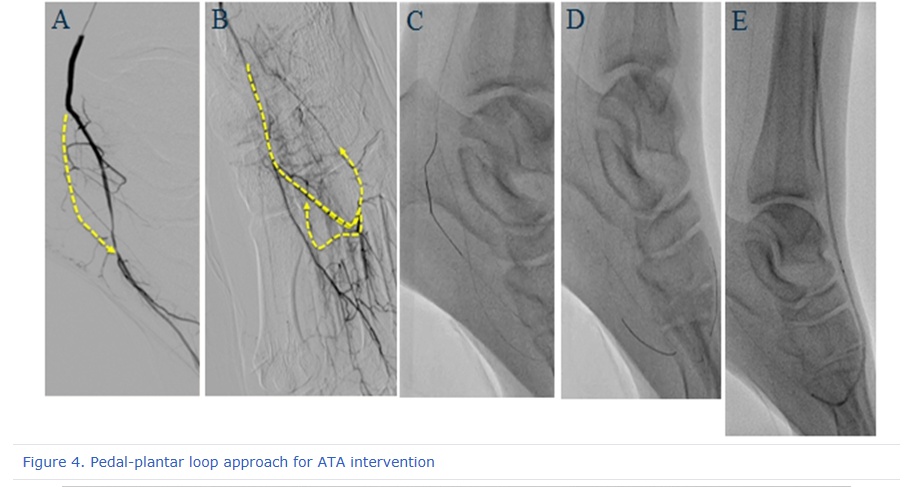
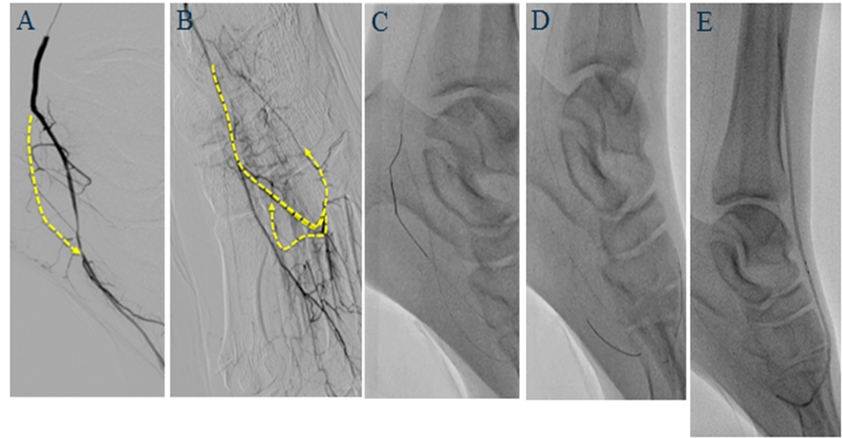
Because the landing zone of the dorsalis artery was not observed, we considered to attempt ATA intervention through pedal-plantar loop access. Initially, we tried an antegrade navigation to stumpless CTO of left lateral plantar artery using an Armada XT OTW balloon and Regalia guidewire (Fig.4-A), but, failed. We approached it in the retrograde direction to proximal lateral plantar artery via small connection between medial and lateral plantar arteries (Fig.4-B,C). Based on retrograde guidewire located at the proximal lateral plantar artery, antegrade navigation of lateral plantar CTO was successfully done (Fig.4-D). Then, balloon angioplasty for lateral plantar was done using a 1.5x20mm balloon catheter.
{kind=link}
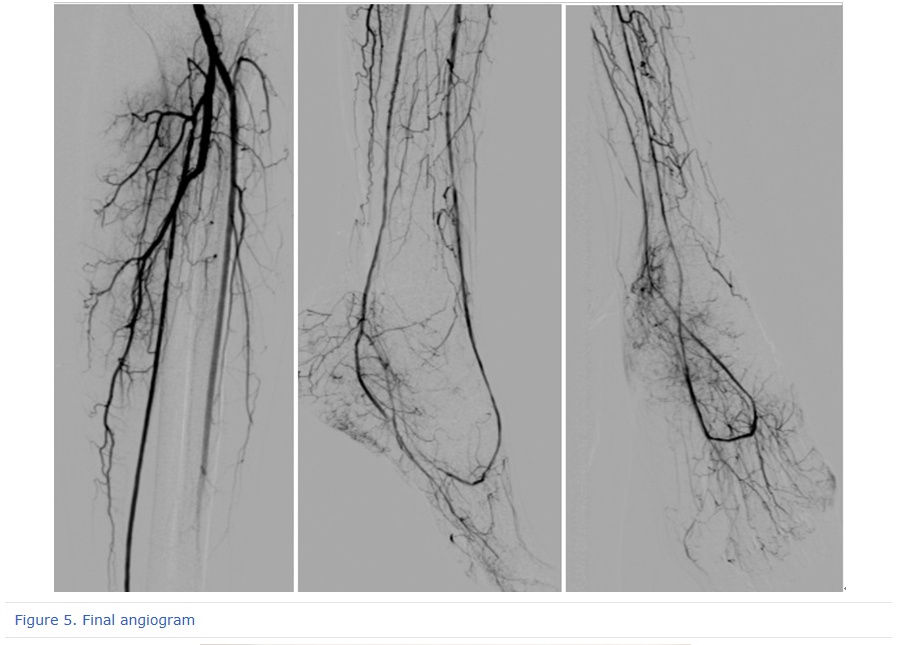
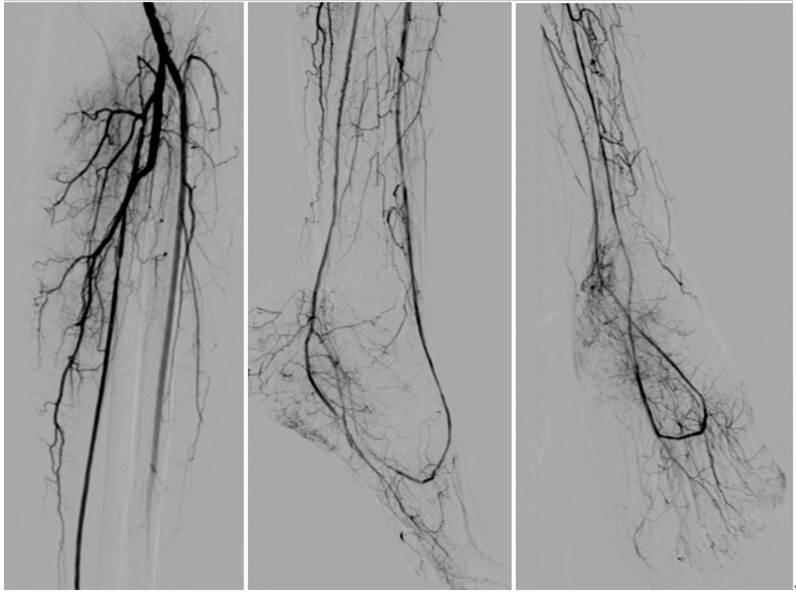
Pedal-plantar loop access was performed for dorsalis-ATA retrogradely with an Armada XT OTW and a Regalia guidewire. Retrograde guidewire was externalized through ATA CTO and the sheath. Balloon angioplasty for whole ATA-dorsalis was done with a 2.0/2.5x210mm tapered balloon catheter (Fig.4-E). Repeated balloon angioplasty for whole PTA-lateral plantar-pedal loop was done with a 2.0/2.5x210mm tapered balloon catheter. Final angiogram showed less than 20% residual stenosis at the ATA and PTA. The pedal-plantar loop flow was well opened with prompt blood supply to the foot (Fig.5).
{kind=link}
Given the clinical diagnosis of thromboangiitis obliterans, the patient was educated on the importance of smoking cessation, and treated with cilostazol and calcium channel blocker. Two weeks later, in the outpatient clinic, we were able to confirm that both pedal pulse were intact, foot wound was healed and the pain improved.
Application of various retrograde procedure, such as pedal puncture, transcollateral and pedal-plantar loop approach, is valuable in a CLI patient with BTK total occlusion that was difficult for antegrade approach.
 |
|
Fig. 1. Left 2nd toe gangrene |
 |
|
Fig. 2. Failed ATA recanalization at outside hospital |
 |
|
Figure. 3. Retrograde approach for PTA intervention |
 |
|
Figure 4. Pedal-plantar loop approach for ATA intervention |
 |
|
Figure 5. Final angiogram |
 |
|
Figure 6. Left 2nd toe wound recovered after 2 weeks |
- 학회소개
- 학술 행사
- 학회지(KCJ)
- 심장학
최신지견 따라잡기
- 진료지침
- 자료실
- 회원공간
- 공지사항