| A 79-year old man was referred to our heart center for dizzines and syncope. He had been on medication for angina pectoris, essential hypertension and diabetes mellitus.
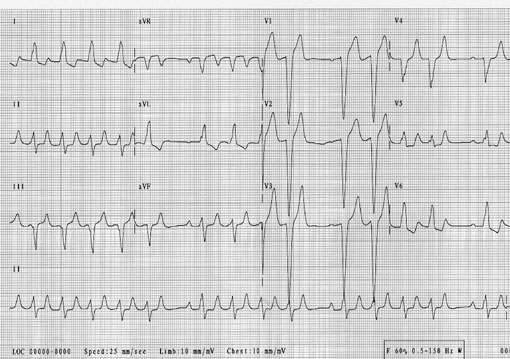
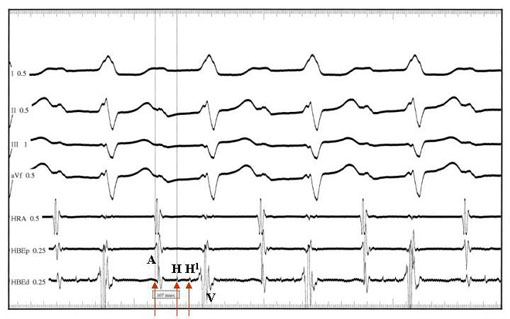
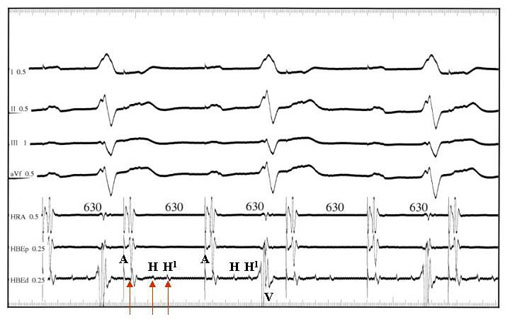
Physical examination disclosed no significant abnormality except grade II systolic murmur at the right upper sternal border. ECG taken on admission showed normal sinus rhythm with prolonged PR interval and 2 beats with LBBB morphology (Fig. 1). On second hospital day, he complained dizziness, 12-lead ECG was recorded demonstrating sinus tachycardia with intermittent drop of QRS complex and LBBB in addition to preexisting PR prolongation (Fig. 2). We thought that syncope of this patient should be caused by paroxysmal high grade AV block. We performed electrophysiology study to evaluate the electrophysiologic function of the sinus node and AV conduction system and implanted a permanent pacemaker based on results of the electrophysiology study (Fig. 3 and 4) and his clinical symptom.
His final electrophysiologic diagnosis was first degree AV nodal and intra-Hisian block and intermittent second egree (or probably high grade) infra-Hisian block presenting with dizziness and syncope.
|